
遊戲教學:提升醫學生的性別素養與促進同志友善醫療
醫學教育者如何善用教學方法,在教導學生專業學習之際,亦培育學生的性別素養?致力於性別與醫學教育研究的高雄醫學大學教授楊幸真,在〈教育為先:促進同志友善醫療的素養導向課程與遊戲教學〉論文中,分享如何在素養導向醫學教育觀點下,運用遊戲教學,創造一個具吸引力的教學活動,促進學生積極參與學習及提升學生的性別素養。
設計遊戲,教性別也教精神醫學
遊戲學習,是一種參與式的教育取徑,能讓學生一起腦力激盪,解決問題。該研究以精神醫學臨床教育醫學生為研究對象,設計「同志醫療與身心健康」課程及九宮格遊戲。九宮格遊戲除了做為暖身活動,引發學生學習動機外,亦做為學習評量工具,具有前測與形成性評量的功用。九宮格遊戲問題的設計,依循素養導向醫學教育的理念,從知識、態度與技能面向出題,了解學生對於同志醫療及精神健康議題方面的認識。
因為是遊戲,即使不會,也是令人愉快的挫敗感
素養,必須透過學習歷程才可能形成,無法直接灌輸。該研究從學生的回應發現,遊戲教學確實能協助教師整合性別與醫療健康照護知識於遊戲過程之中。更重要的是,對於同志醫療與健康議題而言,因為是遊戲,也較能去除學生給予政治正確的回答,能讓學生對於LGBT的認識,包括正確、錯誤、甚至是偏見,都能在遊戲過程中表露與對話,並藉由互動對話產生有意義的學習。
研究者與授課教師在設計九宮格問題時,原以為有些基本知識是學生一定知道且能夠回答的問題。但是,大多數醫學生不知道同性戀去病化是那一年,許多人不清楚何謂跨性別,以及少數人不知道LGBT代表的內涵。好的遊戲學習,具備挑戰性及令人愉悅挫敗感的特性。因為是遊戲,學生即使答不出來,也不會有挫折感。這種在遊戲之中經歷的挑戰與愉快挫敗感,反而更激發學生學習動力。如學生所言: “就更想知道其他題目是什麼”, “吸引我的注意力”,不僅對於接續的性別與精神醫學概念講解更能專注聆聽,亦達到遊戲學習「探索」的功用,激發學生願意主動思考。
此外,做為教學活動與評量工具的九宮格遊戲,還具有支持學習與教學的功用。前者能發現學生的學習困難或迷思概念,以便適時提供學習鷹架,提升效能感。例如,該課程在遊戲進行之後進行概念教學,其中就包含對於同性戀去病化歷史及LGBT的介紹。課程亦安排同志敘說自身就醫經驗,藉由真實生命經驗敘說,以回應九宮格的問題,促進知識、態度與技能的統整學習。後者乃指遊戲的設計,易讓教師將評量融入教學,使評量成為教學方法與教學活動的一部分,而不是外加於教學的評價工具。
學習成效的提升,必得有策略地運用教學方法
該研究發現,遊戲讓學生有參與感,有效提升學生的學習動機及助益主動學習及知識探索。遊戲同時做為教學活動與評量工具,能落實素養導向教育重視學習過程中的評量與立即回饋。運用遊戲教學,確實能有效引領醫學生學習性別,促進將性別知識、態度與技能等多元能力統合納入精神醫學教育與學習之目標。
本校主要研究者之簡介:高雄醫學大學性別研究所教授楊幸真
研究聯繫Email: yhc@kmu.edu.tw
期刊出處:
Yang, H. C. (2019). Education first: Promoting LGBT+ friendly healthcare with a competency-based course and game-based teaching. International Journal of Environmental Research and Public Health, 17(1), 107; https://doi.org/10.3390/ijerph17010107
研究全文下載:https://reurl.cc/Y6dxEO
Game-Based Teaching: Enhancing Medical
Students’ Gender Competency and Promoting LGBT Friendly Healthcare
How can medical educators make good use
of teaching methods to cultivate medical students’ gender competency while
teaching students psychiatry and healthcare education? Yang Hsing-Chen, a
professor at Kaohsiung Medical University(KMU), who is devoted to the study of
gender and medical education, responded to this question in her paper
“Education First: Promoting LGBT Friendly Health Care with a Competency-Based
Course and Game-Based Teaching.” Using the competency-based medical education
(CBME) perspective and gender courses in psychiatric clinical education, this
research paper explored whether the application of game-based teaching
activities can promote gender learning and improve the gender competency of
students.
Design games to teach gender and
psychiatry
Game-based teaching and learning is a
participatory educational approach in which students brainstorm together to
solve problems. The research course, LGBT Health and Medical Care (LGBT HMC) was
added to KMU psychiatric clinical education training for one academic year.
According to the competency-based course and teaching design ideas, a 3 ×
3-grid game was designed as the warm-up game for LGBT HMC. Apart from
stimulating learning motivation, this game served as an evaluative tool,
functioning as a pretest and formative evaluation. The aim of this game was to
prompt learning motivation. It was designed to assess students’ prior LGBT
knowledge–, which provided feedback informing the adjustment of the course and
the improvement of learning conditions. Those questions of the 3 × 3 grid game
were designed to elicit responses regarding students’ understanding of LGBT
health care and mental health issues and could be answered from the
perspectives of knowledge, attitudes, and skills.
“It’s a game, even if you don’t know
the answer, it’s a pleasant frustration”
Using the 3 × 3 grid game as the
teaching activity aimed to achieve two objectives: to trigger the learning
motivation of students and encourage them to proceed to concept learning and to
prevent lecturing on LGBT concepts from becoming an instance of the “banking
education.” Because competency can only be formed through learning processes
rather than through direct inculcation. Student responses revealed that
game-based teaching can help teachers to convey and integrate gender and
medical knowledge or concepts into a game; students can connect with the course
content and experience knowledge transformation to achieve positive learning
outcomes. With respect to LGBT medical and health care issues, within the
context of a game, students were able to express and discuss their correct,
incorrect, or even biased understanding regarding LGBT communities without
being overly concerned with providing politically correct answers. These
interactions and dialogues led to meaningful learning.
When Professor Yang and her researcher
team and the teachers were designing the questions for the 3 × 3 grid game, the
answers to some of the questions were considered basic knowledge that students
must know and be capable of understanding. Surprisingly, none of these
students, who had already commenced their internships in a hospital, could
state the year in which homosexuality was removed from the classification of
mental diseases. Numerous students did not know what “transgender” meant, and a
few students were unfamiliar with the meaning of LGBT. As previously stated,
successful game-based learning is adequately challenging and pleasantly
frustrating. Experiencing challenges can also be positively stimulating in a
game and provoke learning motivation among students; for example, one student
stated that “You become curious about what the other questions are, and that
draws my attention.” The students were more focused and invested in the
following section of the course, which explained the concepts of LGBT health
issues and psychiatry. The game achieved the exploratory function of game-based
learning and provoked active thinking in students.
This study revealed that the 3 × 3 grid
game, which served as the teaching activity and assessment tool, also supported
learning and teaching. The game helps with learning by identifying difficulties
and misconceptions experienced by students, and this enables the timely
provision of instructional scaffolding to enhance efficacy. For example, the
course was designed to conduct concept teaching after the game, and the
concepts included the history of the removal of homosexuality from the
classification of mental diseases and an introduction to LGBT communities. The
teachers also invited LGBT individuals to the class to share their own medical
experiences. These real-life experiences gave the answers to the questions in
the game and helped the students with the integration of knowledge, attitudes,
and skills. In addition, the game helps teaching because the design of the game
facilitates the integration of assessment into teaching, which makes the
assessment part of the teaching method and teaching activity rather than a
supplementary evaluative tool. In fact, both aspects of the game can enhance
assessment for teaching and exhibit the value of the instant feedback obtained
in CBME and game-based learning.
Use teaching
methods strategically to improve learning effectiveness
The findings of this study were as
follows: (1) Games encouraged student participation and benefited gender
knowledge transmission and transformation through competency learning. (2)
Games embodied the idea of assessment as learning. The enjoyable feeling of
pressure from playing games motivated students to learn. Using games as both a
teaching activity and an assessment tool provides the assessment and instant
feedback required in the CBME learning process. In short, game-based teaching
successfully guides medical students to learn about gender and psychiatry
and achieve the learning goal of
integrating knowledge, attitudes, and skills.
Main
researcher: Professor Hsing-Chen Yang,Graduate Institute of Gender Studies,
Kaohsiung Medical University
Author
Email: yhc@kmu.edu.tw
Paper
cited from:
Yang, H.
C. (2019). Education first: Promoting LGBT+ friendly healthcare with a
competency-based course and game-based teaching. International Journal of
Environmental Research and Public Health, 17(1), 107; https://doi.org/10.3390/ijerph17010107
Research
Paper available online on website: https://reurl.cc/Y6dxEO
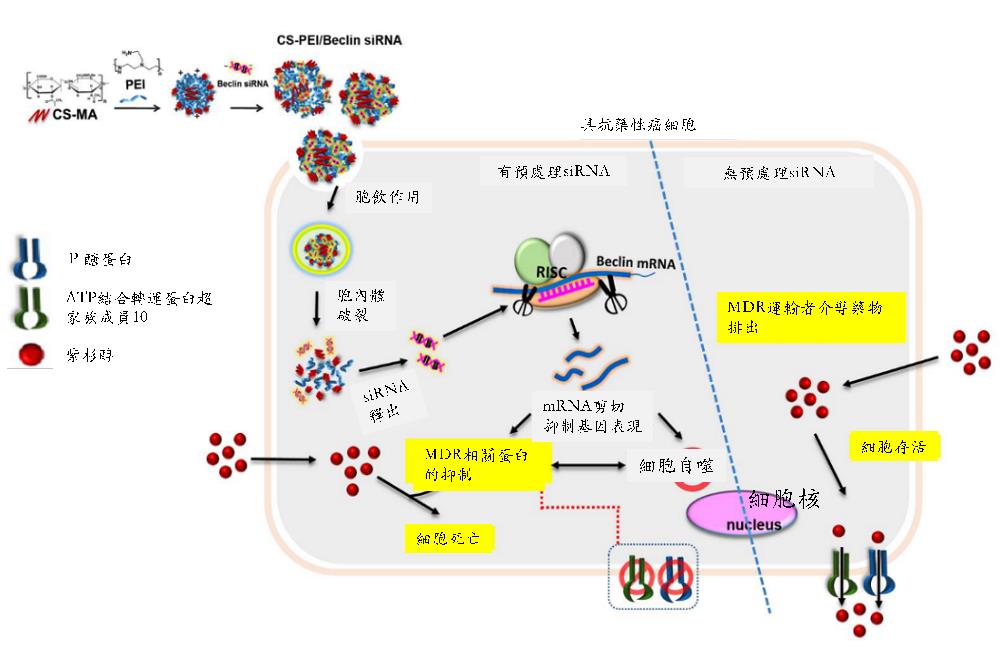
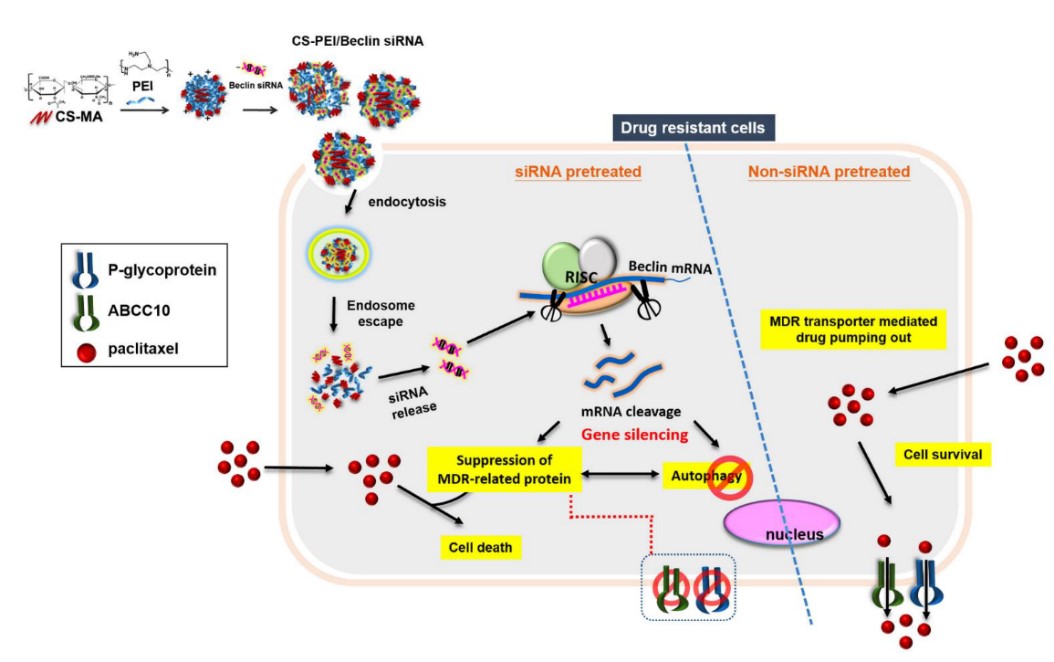
將聚乙烯亞胺(Polyethylenimine, PEI)修飾到硫酸化軟骨素(Chondroitin sulfate, CS),形成一個PEI 接枝CS 之共聚物(簡稱CS-PEI)。PEI是目前市售的一個黃金商品,具高轉染效能的非病毒式基因載體,但是PEI 所擁有的高正電荷密度也對細胞造成很高的毒性。本研究利用低分子量的PEI 接枝到天然的多醣體CS之側鏈上,一來解決臨床未來使用高分子量的PEI對細胞造成的毒性問題;二來以螞蟻雄兵之優勢,利用接掛多條低分子量PEI,使其仍然保留對基因的高轉染率。由於CD44常被發現於腫瘤細胞上,而CS可以辨識細胞膜表面的CD44受體,利用CS-PEI做為基因藥物載體,將增加CS-PEI攜帶之任何基因藥物對細胞表面過度表現CD44的腫瘤或腫瘤幹細胞的靶向性,經由CD44介導的胞飲作用,有效地進入細胞內,提高基因藥物在癌細胞的轉染效能。本研究即以這個低毒性、高轉染的CS-PEI來做為調控自噬作用的Beclin siRNA基因遞送載體;並以紫杉醇(Paclitaxel, PTX)抗藥性的腫瘤細胞株做為細胞模型(如肺癌NCI-H23-TXR),期待藉由抑制細胞的自噬作用,來恢復PTX對腫瘤組織的抑制生長效果。結果發現Beclin siRNA不但抑制Beclin蛋白表現,同時也抑制數個多重抗藥性蛋白的表現,進而促使PTX有效地抑制腫瘤組織的增生。本研究同時也建立一套利用斑馬魚植入腫瘤,快速篩選藥物抑制腫瘤生長的測試平台,未來此平台可延伸至其他腫瘤植入的動物模型。除此,本研究使用的基因載體材料CS-PEI已經獲准台灣專利(I434934)及美國專利(US 8,445,025 B2; US 8,716,399 B2; US 9,050,362 B2),顯見此材料開發具有相當優越的市場開拓新契機。
本校主要研究者之簡介:
本校醫藥暨應用化學系王麗芳教授領導的團隊,集結醫藥化學、生物醫學、奈米醫學、生醫工程、臨床醫學等跨領域專業人才,從化學合成、基因載體的設計、MDR細胞株的建立、自噬作用基因表現、班馬魚腫瘤植入之建立等等,是一個成功的跨系、院、校的成功例子。研究經費由科技部與高雄醫學大學共同支持。
研究聯繫Email: lfwang@kmu.edu.tw ; cchiu@kmu.edu.tw
期刊出處: Molecular Therapy: Nucleic Acids, 2019, 17(9), 477-490.
期刊線上參閱網址:
https://www.cell.com/action/showPdf?pii=S2162-2531(19)30180-5
Polyethyleneimine (PEI) is one of leading cationic polymer for gene delivery because of its high transfection efficiency. However, PEI induced high cytotoxicity due to the positively charged surface characteristics. Herein, we grafted PEI onto chondroitin sulfate (CS) to yield CS-PEI which not only showed transgene efficiency, but reduced PEI cytotoxicity. CD44 is overexpressed in many solid tumor cells. It has been found that CS has the potential to be internalized into cells via CD44-mediated endocytosis. Thus, using CS-PEI as a gene drug delivery system, actively targeting to CD44-overexpressing cancer cells is an ideal approach to enhance transgene efficiency. Multidrug resistance (MDR) is the major obstacle in limitation of therapeutic efficacy of Paclitaxel (PTX). PTX-resistant non-small-cell lung cancer cell line (NCI-H23-TXR) was established and CS-PEI/Beclin-small interfering RNA (siRNA) was constructed to restore sensitivity of PTX against NCI-H23-TXR. Results revealed that knockdown of Beclin simultaneously inhibited MDR-related proteins, and renewed the sensitivity of PTX against NCI-H23-TXR. In vivo study showed that pre-transfection with CS-PEI/Beclin-siRNA followed by PTX treatment decreased the tumor size in NCI-H23-TXR zebrafish xenografts. (Taiwan Patent No. I434934; United States Patent US 8,445,025 B2; US 8,716,399 B2; US 9,050,362 B2)
Main researcher Intro.
Dr. Li-Fang Wang, a professor of Department of Medicinal and Applied Chemistry at Kaohsiung Medical University.
Author Email: lfwang@kmu.edu.tw ; cchiu@kmu.edu.tw
Paper cited from: Molecular Therapy: Nucleic Acids, 2019, 17(9), 477-490.
Paper online website:
https://www.cell.com/action/showPdf?pii=S2162-2531(19)30180-5
量身訂做的教育介入提升兒童癌症存活者之健康行為自我效能
治療和照護的進步雖然提高癌症兒童的存活率,但兒癌存活者仍須面臨癌症和治療相關不利健康的結果。約60%的兒癌存活者至少罹患ㄧ種長期合併症,其中80%存活者的合併症需要接受治療。因此提高兒癌存活者徵狀管理之自我效能和健康促進行為,將有助於提高其自我效能,進而採取健康的生活方式。因此,規劃兒癌存活者的健康促進策略就顯得特別重要。
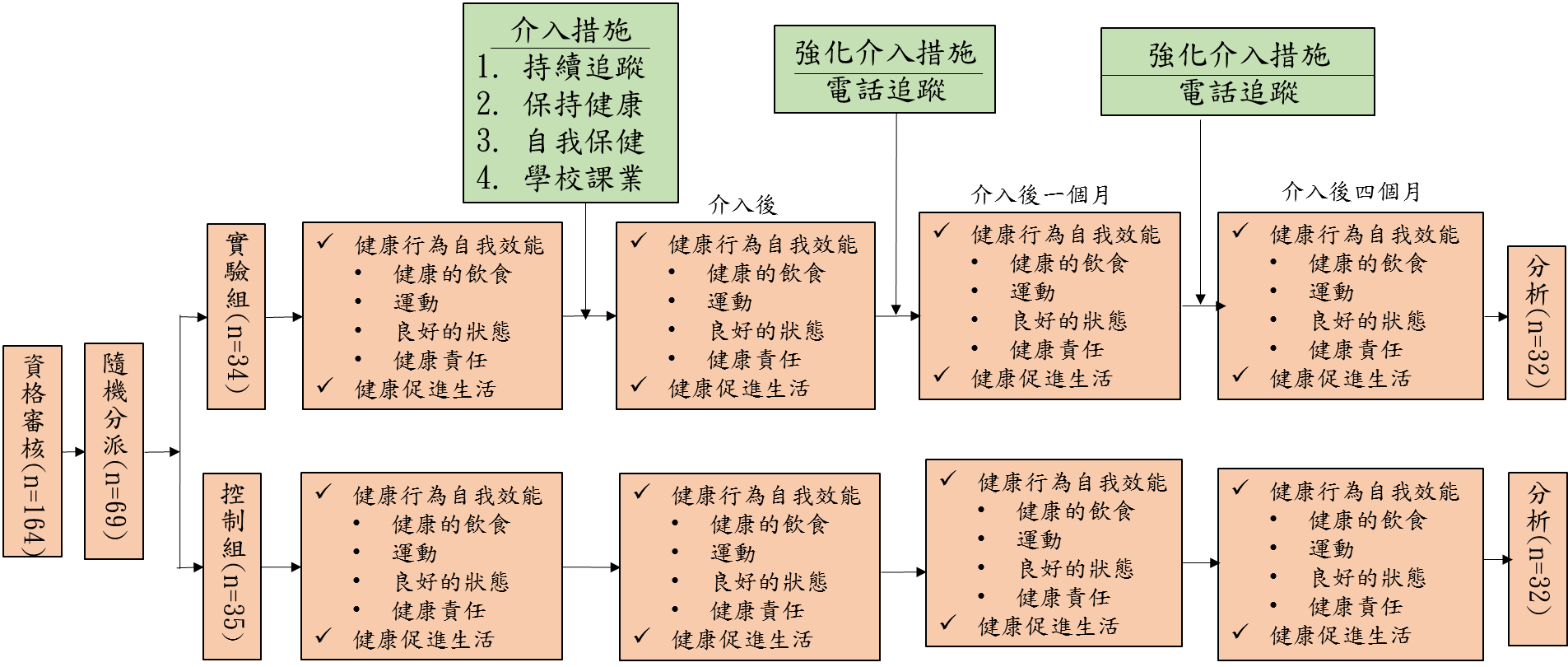
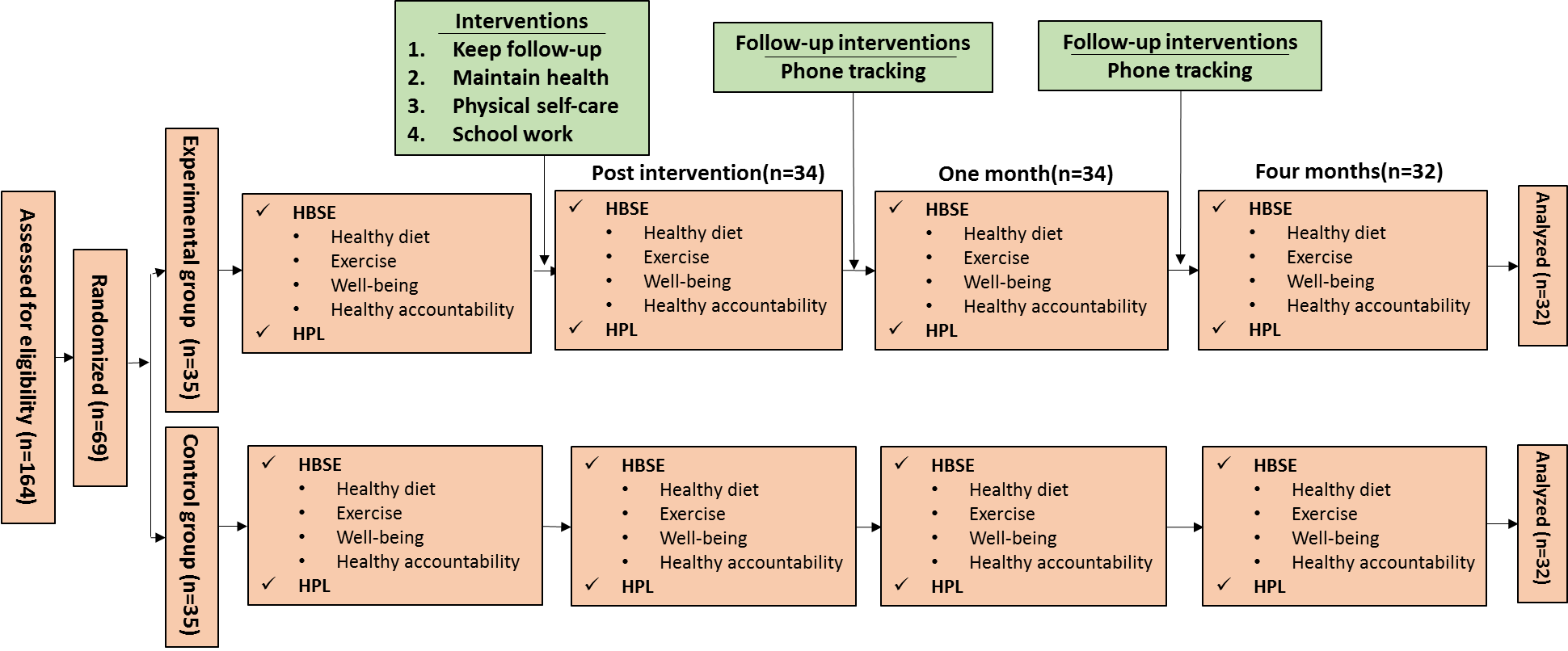
本研究為隨機重複測量試驗,利用自我效能理論,首創兒童癌症存活者衛教課程,內容包含:建立自我意識(了解疾病和治療的潛在副作用)、預防健康(飲食和運動)和促進健康(自我照顧和重返學校)。全程共設計6次活動,於一周結束,每次進行約45-60分鐘,並於衛教介入後一個月,4個月電訪追蹤,以提升兒癌存活者健康行為自我效能。
結果顯示實驗組在健康行為自我效能和健康促進生活得分隨著時間而顯著增加(all p < 0.05),且教育介入後4個月的健康行為自我效能得分顯著高於對照組(F= 5.32, p= 0.02, η2= 0.25),控制組在健康行為自我效能並未隨著時間顯著性改變。研究對象給與介入措施很高的評價(M=9.29)。本研究亦發現運動是癌症兒童存活者最大的障礙,設計簡單可行的運動,並能在住院期間執行,以及增加運動意願和持續的動機,都是未來努力的方向。未來研究可持續評值教育介入的長期效果,以及可能的聯動效益。
透過隨機對照且持續追蹤4個月的實驗性研究設計,研究結果發現量身訂做的教育介入,可以提升兒癌存活者的健康行為自我效能進而促進健康生活型態
本校研究者之簡介:
1. 吳麗敏 高雄醫學大學護理學系教授兼系主任
2. 許心恬 高雄醫學大學護理學系副教授
3. 劉 怡 高雄醫學大學護理學系副教授
4. 蘇秀蘭 高雄醫學大學附設中和紀念醫院專科護理師
研究聯繫Email:painting@kmu.edu.tw
期刊出處:
Li-Min Wu, Chin-Mi Chen, Hsin-Tien Hsu, Fan-Ray Kuo & Hsiu-Lan Su. (2019).
Tailored education enhances healthy behavior self-efficacy in childhood cancer survivors: A ramdomised controlled study with a 4-month follow up.
研究全文下載:
Tailored education enhances healthy behaviour self‐efficacy in childhood cancer survivors: A randomised controlled study with a 4‐month follow‐up
This study was to evaluate the acceptability and effectiveness of a tailored education on healthy behaviors self‐efficacy (HBSE) and health promotion lifestyle (HPL) for childhood cancer survivors. A two‐group, randomized study with repeated measures was conducted in Taiwan. Participants were randomly assigned to receive six 45–60 min individual education and follow‐up telephone counselling sessions (n = 34) or standard of care only (n = 35). Each participant was assessed with HBSE and HPL questionnaires and was evaluated at three time points (at baseline, and then 1 and 4 months after intervention). The attrition rate was 7.2%. HBSE and HPL scores increased across the three time points in the experimental group (all p < 0.05), except for the HBSE exercise subscale (p= 0.85). HBSE scores were significantly higher for the experimental group than for the control group after 4 months of intervention (F = 5.32, p = 0.02, η2 = 0.25). No significant improvements in HBSE were observed over time in the control group. The intervention was acceptable and effective in promoting HBSE in childhood cancer survivors. Further empirical work is needed to reveal the effects of the intervention over a longer period of time and to improve patient engagement in exercise.
A tailored education can improve childhood cancer survivors’ health behavior self-efficacy by conducting the randomized controlled study with a 4‐month follow‐up
Main researcher Intro.
https://pubmed.ncbi.nlm.nih.gov/31020742/
Researcher
1. Li‐Min Wu RN, PhD, Professor, chair, School of Nursing, Kaohsiung Medical
University, and Department of Medical Research, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
2. Chin‐Mi Chen RN, PhD, Associate Professor, Department of Nursing, Fu Jen Catholic
University, New Taipei City, Taiwan.
3. Hsin‐Tien Hsu RN, PhD, Associate Professor, School of Nursing, Kaohsiung Medical
University, and Department of Medical Research, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
4. Yi Liu RN, PhD, Associate Professor, School of Nursing, Kaohsiung Medical
University, Kaohsiung, Taiwan.
5. Hsiu‐Lan Su RN, MSN, Nurse Practitioner, School of Nursing, Kaohsiung Medical
University, and Department of Medical Research, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
Author Email: painting@kmu.edu.tw
Paper cited from:
Li-Min Wu, Chin-Mi Chen, Hsin-Tien Hsu, Fan-Ray Kuo & Hsiu-Lan Su (2019). Tailored education enhances healthy behavior self-efficacy in childhood cancer survivors: A ramdomised controlled study with a 4-month follow up.
Research Paper available online on website
三陰性乳癌新進展-奈米級白蛋白載體新藥
有「乳癌殺手」之稱之三陰性乳癌好發於40歲前,且其來自於名為BRCA-1基因所發生之變異疾病,也是讓女星安潔莉娜裘莉發現自己具有BRCA基因變異後,選擇切除乳房作為預防癌症發生之主因,近年來透過癌細胞基因解密讓乳癌分類更加明朗化,乳癌基因表現大致分為三類:雌激素受體(ER)、黃體素受體(PR)、人類上皮生長受體第二對(HER-2),如癌細胞三種基因表現皆為陰性則歸類為「三陰性乳癌」,目前是臨床上治癒率最低、復發率最高之乳癌類型,導致選用標靶藥物存在諸多限制,病患仍使用化學治療為主。
近日,高雄醫學大學方逸萍副教授及其研究生林欣哲之論文刊登於國際知名藥劑領域期刊,研究中指出「抗癌藥SN-38 白蛋白奈米載體」是針對三陰性乳癌新劑型藥物,SN-38為有強大抗癌活性之喜樹鹼衍生物,但因難溶於水且副作用大等特性限制了其於臨床上之應用;為此,方老師研究團隊藉由研發白蛋白奈米載體結合SN-38之技術克服其於臨床使用限制。白蛋白為人體內生性蛋白所構成,是血漿中最豐富蛋白質、能維持血漿滲透壓、運送血液營養物等,除了是人體中不可或缺之蛋白質外,也容易被代謝且不易致敏,利用白蛋白結構中之親水性及親脂性特質,可有效將SN-38包裹在奈米粒子之間。方老師研究團隊所合成之「抗癌藥SN-38 白蛋白奈米載體」經細胞實驗證實:可有效抑制三陰性乳癌細胞株生長,且白蛋白奈米粒子可增加SN-38進入癌細胞之有效劑量,且SN-38從奈米粒子釋出後更可標靶精準毒殺癌細胞。
乳癌有逐漸年輕化之趨勢,多數年輕患者在發現乳癌當下,家庭與事業皆處於黃金時期,一旦確診三陰性乳癌除了生理上不適,心裡也會帶來諸多壓力,期待新劑型開發能順利進行,未來上市後作為治療三陰性乳癌之新選擇。 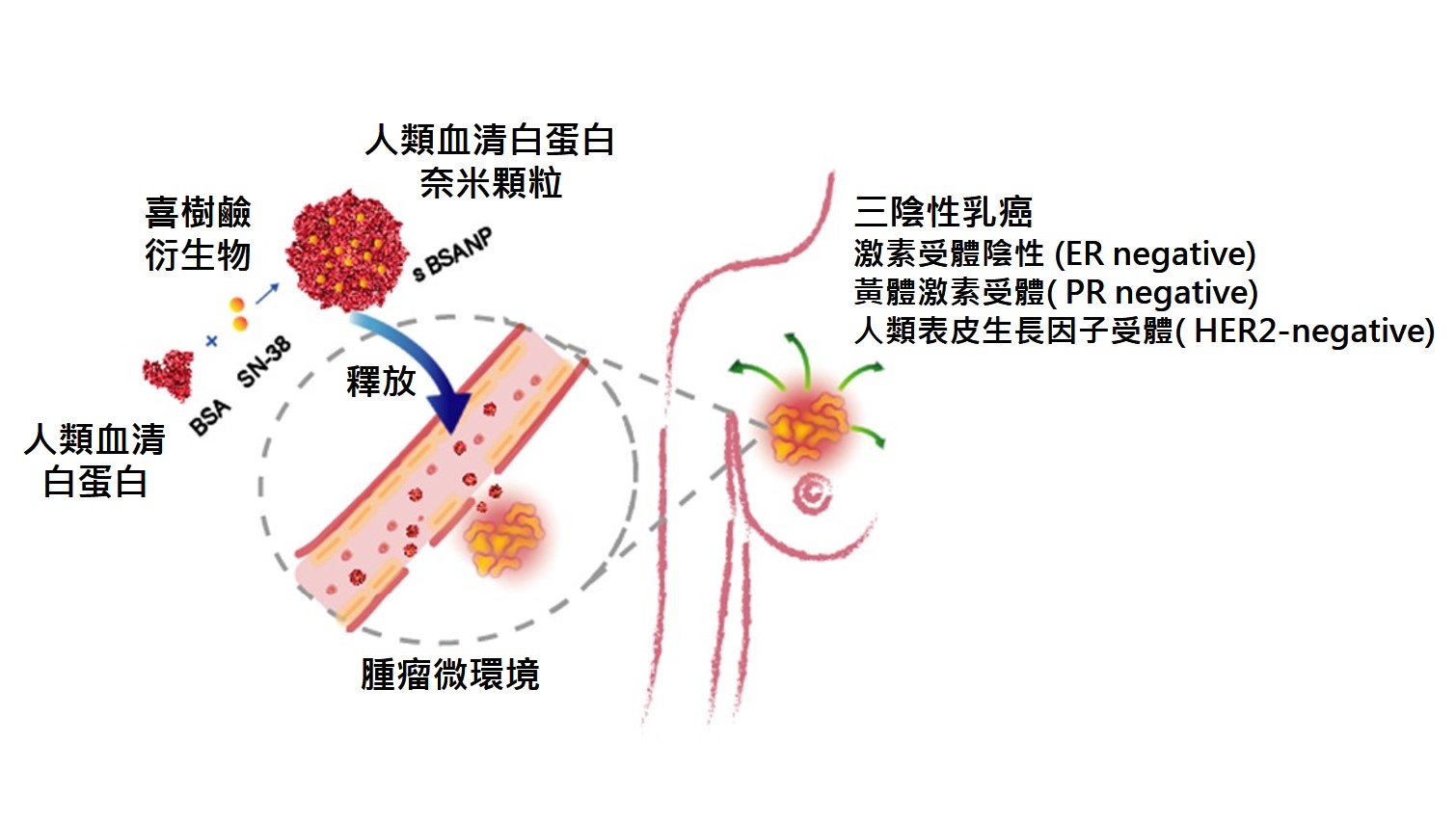
本篇為高雄醫學大學2019年月傑出論文11月份得獎文章,代表作者為藥學系方逸萍副教授。
本校主要研究者之簡介
研究聯繫Email:
ypfang@kmu.edu.tw
期刊出處:
Pharmaceutics 2019, 11, 569
期刊線上參閱網址:
The Progress in Triple Negative Breast Cancer Research Continues: the albumin nano drug carrier
Triple negative breast cancer (TNBC), related to BRCA1 mutation, is an aggressive breast cancer common in female younger than age 40. Potentially being in the TNBC population, the actress Angelina Jolie made the difficult decision to undergo a preventative mastectomy due to the alarming nature of TNBC. Lacking estrogen receptor (ER), progesterone receptor (PR) and HER2 receptor, TNBC has limited options on targeted medications, which results in low survival rate and high recurrence among the breast cancer subtypes.
Recently, Professor Yi-Ping Fang with graduate student Hsin-Che Lin in Kaohsiung Medical University published a research on “anticancer agent SN-38 entrapped albumin nanoparticles to TNBC.” SN-38 is a camptothecin derivative with very potent anticancer effect. The clinical application of SN-38, however, is limited by its low solubility and serious adverse effects. For this reason, Professor Fang’s team proposed a solution to combine SN-38 with albumin carrier, considering albumin is not only one of the most abundant protein in human and maintains osmotic pressure, delivers substances in blood circulation, but also can be easily metabolized and further eliminated. By utilizing the natural amphiphilic property of albumin, Professor Fang’s team developed a procedure to formulate SN-38 in albumin nanoparticles which further showed promising targeting effect by accumulation these albumin nanoparticles in TNBC cell line to suppress TNBC cell line growth.
Upon the trend of younger breast cancer diagnosed such as TNBC in this case, majority of breast cancer patients are at their pinnacle of life and career, and this disease only brings serious distress physically and mentally. Through this research, the contribution to the solution to the unmet TNBC clinical need may be expected, with the ultimate goal in mind, to improve TNBC patients’ quality of life.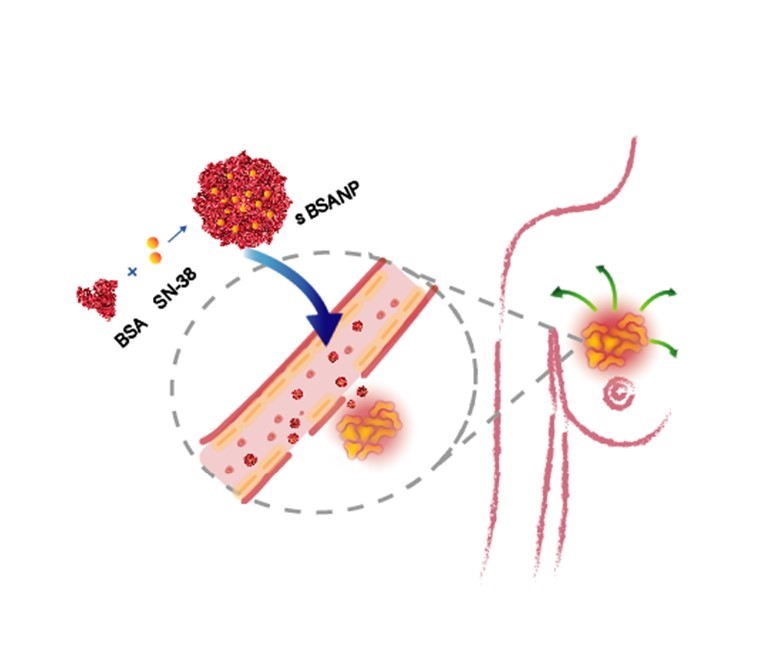
This article-“High Potency of SN-38-Loaded Bovine Serum Albumin Nanoparticles Against Triple- Negative Breast Cancer” , written by Rept. Author Associate Professor Yi-Ping Fang from School of Pharmacy, is award for Kaohsiung Medical University 2019 Monthly Excellent Paper Award in Nov.
Main researcher Intro.
Author Email: ypfang@kmu.edu.tw
Paper cited from: Pharmaceutics 2019, 11, 569
Paper online website: https://pubmed.ncbi.nlm.nih.gov/31683822/
在大多數腫瘤所導致的預後不良及相關死亡中,首要原因(90%)是癌症細胞的轉移所導致。儘管有關於癌症轉移的相關研究日益增多,造成腫瘤轉移的作用機制尚不明確。癌症細胞的轉移是一個複雜過程,而癌細胞的上皮-間質特性轉化(EMT)被認為是最初也是至為重要的步驟。儘管許多信息傳遞分子及路徑(例如,PI3K,Snail,HIF1α,和 SIP1)和轉錄因子(TWIST1/ 2, SNAIL1/ 2,ZEB1/ 2,和 FOXC2)被認為是調節及誘導 EMT 發生的主要因子,詳細的調控機制仍是未知。表觀基因調控(Epigenetic regulation)是癌症進展過程中的重要調節過程,特別是蛋白質乙醯化的機制,但是,其潛在機制亦尚未充分了解。
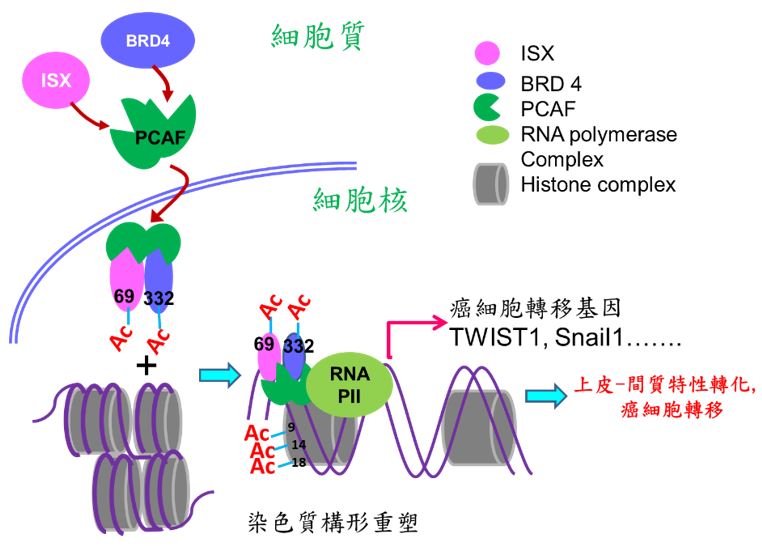
本校醫學研究所許世賢教授利用免疫沉澱法、質譜分析(LC-Mass/Mass)及鄰位連接技術(Proximity Ligation Assay; PLA)等分子生物學技術發現一個新的致癌複合體(ISX-BRD4),此複合體可誘發及參與腫瘤細胞微環境之建構,使腫瘤細胞進行轉移及惡化。箱型基因Intestine -specific homeobox (ISX) 是一個許世賢教授實驗室發現及證實的一個致癌小腸專一性表現之箱型基因,實驗室多年的研究發表中證實此轉錄因子可經由發炎因子(IL-6)所誘發並且高量表現在肝癌細胞及病人組織中。在細胞核中,經由直接結合下游細胞週期因子(cyclin D1)之啟動子,ISX 的表現可調控癌細胞的增生並與病人之生存時間、腫瘤大小及腫瘤期別有著緊密的調控關係。近期研究發現表觀乙醯轉移酶P300 / CBP相關因子(PCAF)可經由調控ISX(K69)與BRD4(K332)複合物之乙醯化,促使ISX-BRD4複合體進入細胞核,與EMT調控基因啟動子結合並進一步乙醯化組織蛋白3(Histone H3; K9, 14, 18),促使染色質雙股結構鬆開,開始EMT相關調控基因轉錄促進癌症轉移。過度表現ISX會增強EMT標記物的表現,包括EMT 調控基因TWIST1,Snail1, Slug, ZEB1和VEGF,以及隨之而來的癌症轉移,但會抑制E-鈣黏著蛋白(E-cadherin)的表現。 在肺癌中,PCAF–ISX–BRD4複合體過度表達與臨床轉移特徵和不良預後呈現高度相關性。這些結果證實,PCAF–ISX–BRD4複合體表現確實加強了EMT信號傳導,並對腫瘤的發生和轉移發揮了調節作用。
論文全文:https://pubmed.ncbi.nlm.nih.gov/31908141/
圖說:根據實驗數據和結構建模的實驗發現,BRD4的BD2域上的酪氨酸(Tyr390)和天冬醯胺(Asn433)殘基是BRD4識別並與ISX的乙酰化賴氨酸(Lys69)結合併促進ISX–BRD4複合物形成所需的關鍵殘基。
本篇為高雄醫學大學2020年月傑出論文2月份得獎文章,代表作者為醫學院醫學研究所許世賢教授。
本校主要研究者之簡介:
許世賢 教授, 高雄醫學大學 醫學研究所
研究聯繫Email:
許世賢教授 (jackhsu@kmu.edu.tw), TEL:07-3121101#2136
期刊出處: EMBO Rep. 2020 Feb 5;21(2):e48795.
研究全文下載:
Cancer directly affects at least one-third of the human population. Despite this extensive research prevalence, the genetic determinants of cancer risk remain largely unknown. Metastasis, a complex, multistep morphogenetic process, refers to the dissemination from a primary tumor mass to distal tissues, with epithelial–mesenchymal transition (EMT) believed to be the initial and vital step. Despite several signaling (e.g., PI3K, snail, HIF1α, and SIP1) and transcriptional (TWIST1/2, SNAIL1/2, ZEB1/2, and FOXC2) factors having been identified as major regulators of EMT, a detailed regulatory mechanism for oncogene-induced EMT has yet to be established. Epigenetic regulation is an important process during cancer progression, however, the underlying mechanisms, particularly those involving protein acetylation, remain to be fully understood. Recently, Prof. Hsu (GIM, KMU) found intestine-specific homeobox (ISX), a newly identified pair-family homeobox transcription factor, is a pro-inflammatory cytokine (IL-6) induced homeobox gene and high expression in hepatoma cells and HCC patients. Through directly regulates downstream cell cycle regulators (cyclin D1 and E2F1), ISX shows high correlation to patient survival time, tumor size, tumor number and progression stage, and accelerated cell proliferation and tumorigenic activity in hepatoma cells which highlights ISX is an important regulator in hepatoma progression with significant potential as a prognostic and therapeutic target in HCC. In addition, the exposure of environmental pollutants will also trigger and exacerbate the occurrence of liver cancer by inducing the ISX and relevant epigenetic genes expression via the function of its upstream regulatory gene-AHR. At the same time, the expression of ISX in HCC cells can also inhibit the host's own immune system through the regulation of immune checkpoint and tryptophan metabolism-related genes to promote the further growth and metastasis of hepatoma cells. Here, we show that P300/CBP-associated factor (PCAF)-dependent acetylation of intestine-specific homeobox (ISX) regulates epithelial-mesenchymal transition (EMT) and promotes cancer metastasis. Mechanistically, PCAF acetylation of ISX at lysine 69 promotes the interaction with acetylated bromodomain-containing protein 4 (BRD4) at lysine 332 in tumor cells, and the translocation of the resulting complex into the nucleus. There, it binds to promoters of EMT genes, where acetylation of histone 3 at lysines 9, 14, and 18 initiates chromatin remodeling and subsequent transcriptional activation. Ectopic ISX expression enhances EMT marker expression, including TWIST1, Snail1, and VEGF, induces cancer metastasis, but suppresses E-cadherin expression. In lung cancer, ectopic expression of PCAF–ISX–BRD4 axis components correlates with clinical metastatic features and poor prognosis. These results suggest that the PCAF–ISX–BRD4 axis mediates EMT signaling and regulates tumor initiation and metastasis.
Full paper linkage: https://pubmed.ncbi.nlm.nih.gov/31908141/
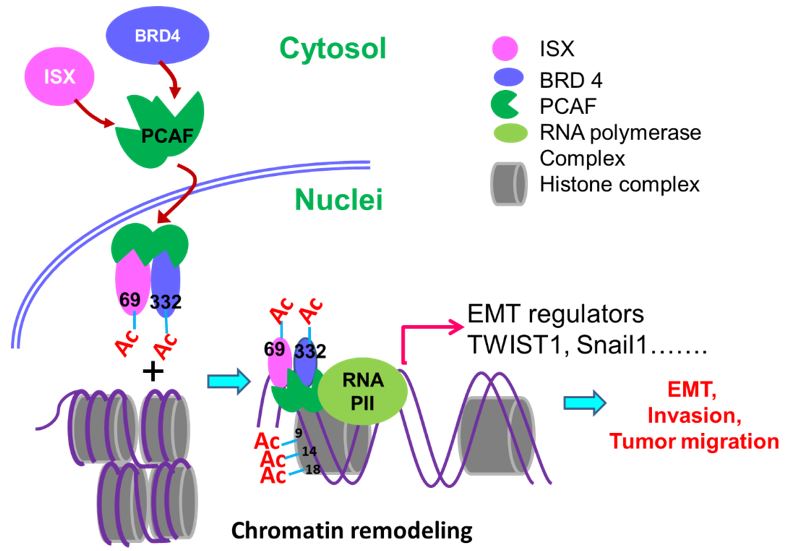
Figure legend: Illustration of experimental data and structure modeling, it is demonstrated that Tyr390 and Asn433 residues on the BD2 domain of BRD4 are critical residues needed for BRD4 to recognize and bind with the acetylated Lys69 of ISX to facilitate the formation of the ISX–BRD4 complex.
Main researcher Intro.
Professor Hsu Shih-Hsien, Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Author Email
Professor Hsu: jackhsu@kmu.edu.tw, TEL:07-3121101#2136
Paper cited from:
EMBO Rep. 2020 Feb 5;21(2):e48795.
Research Paper available online on website:
版權所有 © 2021-2025 高雄醫學大學
